NuDigest
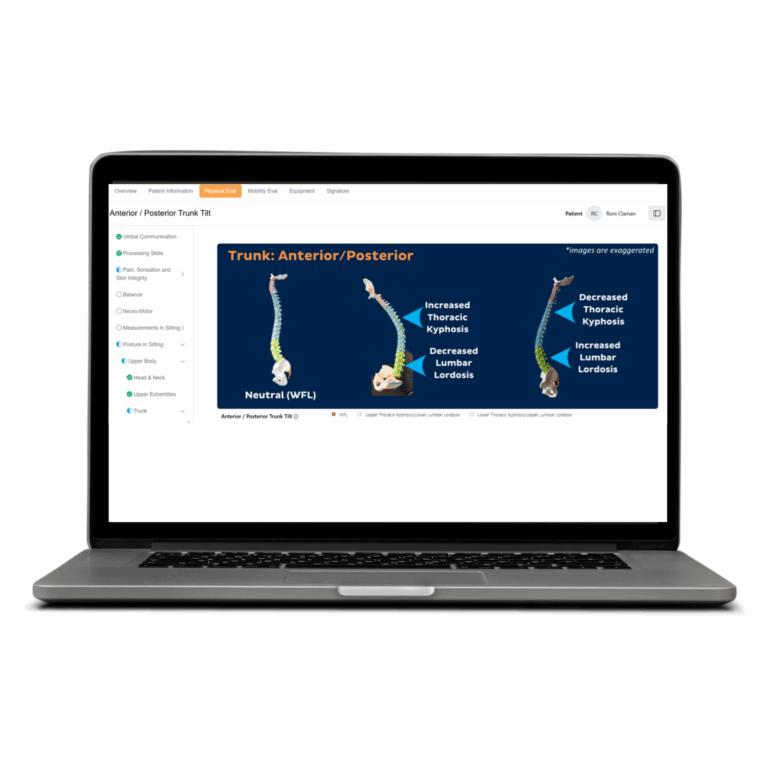
NuDigest offers Numotion customers and medical professionals, with resources as they navigate the ever-changing landscape of CRT. Authored by experts from Numotion and across the industry, each NuDigest provides information on everything from better bladder health to documentation needed to get a chair approved through Medicare.
34 posts